December 5, 2024
How does CAR-T technology work?
In simple terms, it’s a method for enabling our immune system to fight debilitating diseases. CAR-T technology genetically engineers T cells (a patient’s or a donor’s) to express a chimeric antigen receptor targeting a tumor antigen.
CAR-Ts identify and attach to specific antigens on the cancer cell surface (see Figure 1). The CAR-Ts can then proliferate and kill the cancer cells.
The FDA has approved several CAR T-cell therapies including Abecma (idecabtagene vicleucel), Breyanzi (lisocabtagene maraleucel), Kymriah (tisagenlecleucel), Tecartus (brexucabtagene autoleucel), and Yescarta (axicabtagene ciloleucel). These approvals have fueled massive interest because they have revolutionized the drug-disease continuum. Cell therapies have greater durability of efficacy than conventional treatments. Not surprisingly, the FDA has developed a relevant guidance for industry to assist developers.
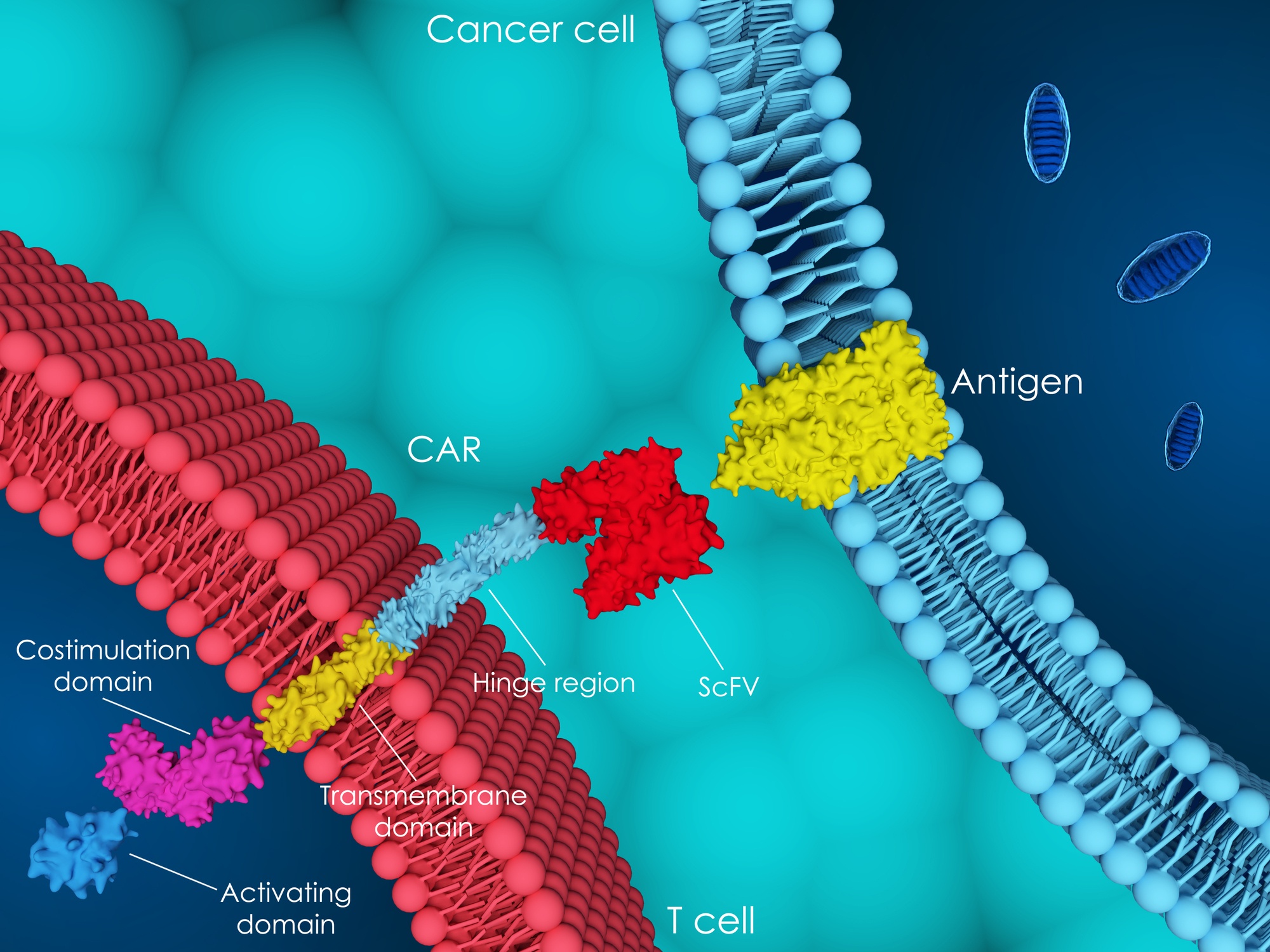
Figure 1. Schematic for how CAR-Ts identify and attach to specific antigens on the cancer cell surface.
The clinicaltrials.gov database contains more than 100-cell therapy investigative treatments in clinical trials. One key aspect of product development is the consistent, within specification, product performance as it relates to chemistry, manufacturing, and scale-up. Cell therapy therapeutics have started to reimagine manufacturing to produce consistently safe and quality medicines.
Why is that? Let’s reflect on this aspect before launching into our 3 key development considerations.
What are the steps in CAR-T therapy?
Once a patient qualifies for the “procedure” (Figure 2) and arrives at the clinic, they undergo leukapheresis to isolate peripheral blood mononuclear cells. At this stage, the “procedure” transitions into a “manufacturing” phase. Thus, the patient undergoes chemotherapy during cellular processing. Genetic material is then transferred through viral vectors following cell expansion. After this step, the cells are infused into the patient following a process of lymphodepletion.
So, manufacturing that occurs in the clinic replaces traditional pharmaceutical manufacturing.
Here are 3 key considerations.
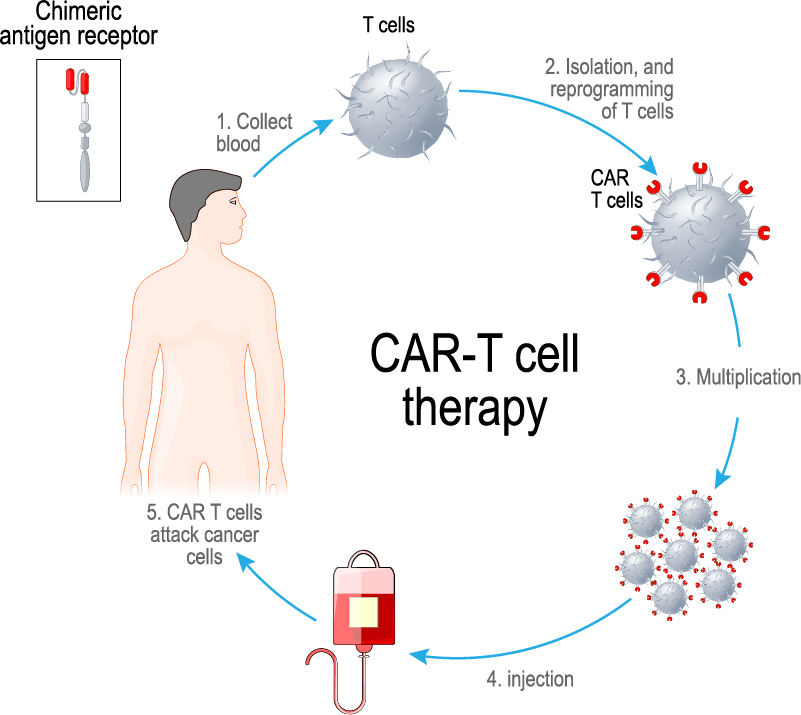
Figure 2. CAR-T cell therapy process
1. Clinical pharmacology strategy for CAR-T Therapeutics
The clinical pharmacology considerations for CAR-T therapeutics ordinarily involve:
- defining the mechanism of action,
- assessing the on-target effects of the therapy, and
- characterizing the cellular kinetics of the new therapy.
Some common translational strategies are to understand cellular kinetics and dynamics and whether biological determinants underpin responders vs non-responders.
For example, let’s take KYMRIAH. It was developed by transducing autologous T cells with a lentiviral vector encoding a chimeric antigen receptor (CAR) composed of a murine single chain antibody variable fragment (scFv) specific for CD19, linked to intracellular signaling domains from 4- 1BB (CD137) and CD3-zeta. Here’s the summary basis of approval. One signaling domain enhances the expansion and persistence of KYMRIAH cells. The other signaling domain initiates T-cell activation and antitumor activity. When CAR binds to CD19-positive target cells, it triggers anti-tumor activity, cellular proliferation, and persistence.
Conventional MIDD tools including population PK models can relate exposure with recovery and tumor burden. Given cellular dynamics is a key concern, adapted cellular kinetic models are usually a better mechanistic model to inform drug development decisions. A good example of a cellular kinetic model is in Figure 3 (Adapted from Ogasawara et al., 2021).
In Ogasawara’s model, these are the following parameters:
- C0 refers to initial transgene levels,
- Cmax is the maximum transgene levels,
- Fβ is the fraction of Cmax that appears in the β or terminal phase,
- HLα the initial (α phase) decline half-life,
- HLβ the terminal (β phase) half-life,
- Tdbl is the doubling time during the growth phase,
- Tgro is the growth phase duration,
- Tlag is the lag phase duration, and
- Tmax is the time to maximum transgene levels.
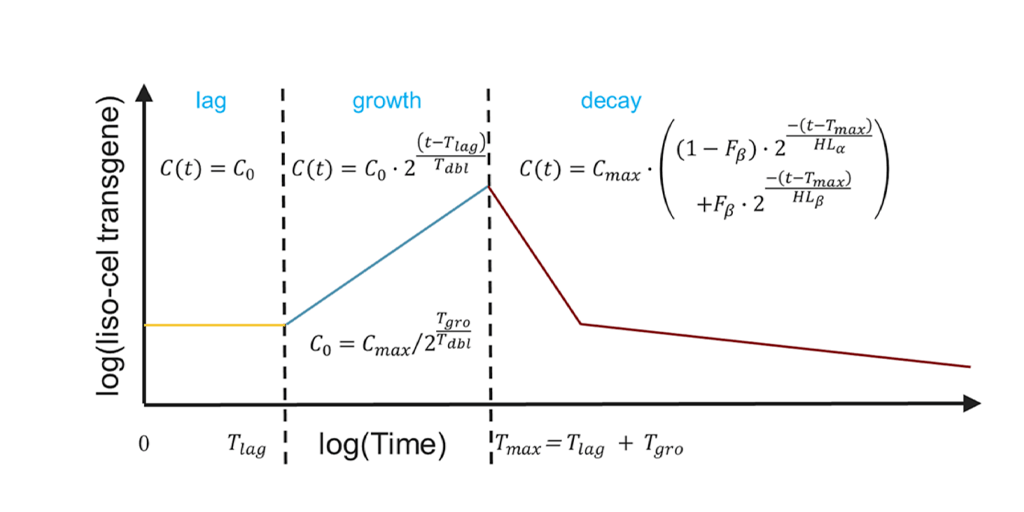
Figure 3: Cellular kinetic model of lisocabtagene maraleucel (Adapted from Ogasawara et al., 2021).
Traditional methods of sample collection may not provide precise characterization of cellular kinetics. Recent attempts in quantifying cellular dynamics have included radiolabeling of CAR-T cells. Dual imaging of tumor and CAR-T cells can assist in interpreting antitumor responses.
3. Cell therapy safety considerations
A cell therapy developer needs to assess many clinical safety considerations of the product. Once administered, the CAR-T cell proliferation rate can determine the extent and magnitude of the key safety issues: cytokine release syndrome (CRS) and neurotoxicity.
These safety issues may be life-threatening and typically arise within 28 days of infusion. CRS or macrophage activation syndrome is “on target” toxicity as the T cells expand and exert their effects. CRS is commonly managed by blocking the IL-6 receptor with tocilizumab.
Two types of neurotoxicity are associated with these products; those that are common and reversible (e.g., aphasia), and those that are much more severe (e.g., fatal cerebral edema). Prolonged B cell aplasia is also a known safety issue with these therapies. Patients often receive intravenous immunoglobulin to manage this complication.
The package insert highlights these safety issues. The example below is from the KYMRIAH® (tisagenlecleucel) package insert.
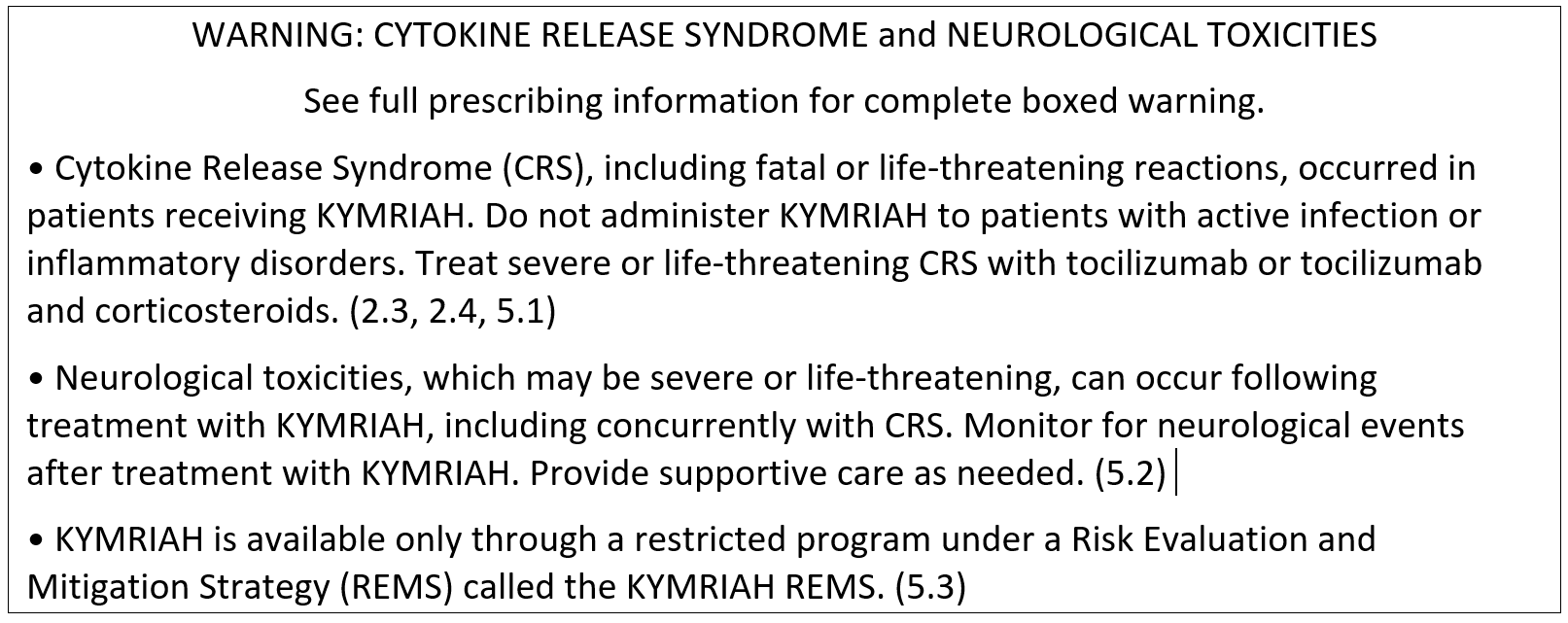
Figure 4
Several other approaches in development use the concept of cell therapy. These are TCRs (T-cell receptor-based therapies) which use the T-cells’ natural ability to recognize antigens. This means they can penetrate tumors and attach both the cancer cell’s inside and surface. In addition, NK (natural killer) cell therapies are coming along, which may address some of the side effects associated with CAR-Ts.
In conclusion, developing CAR-T therapeutics requires a clinical pharmacology/pharmacometrics strategy to elucidate the mechanism of action and explain biological effects concerning efficacy and safety. It also requires an understanding of immunology and cellular biology. Lastly, sponsors need applied mathematical tools to develop a plausible understanding of cellular-level kinetics and dynamics.
Using Clinical Pharmacology & Pharmacometrics to Accelerate Cell Therapy Development: A Patient’s CAR-T Journey
To learn more about best practices for cell therapeutics development, please watch this webinar.
References
Ogasawara K, Dodds M, et al. Population Cellular Kinetics of Lisocabtagene Maraleucel, an Autologous CD19‑Directed Chimeric Antigen Receptor T‑Cell Product, in Patients with Relapsed/Refractory Large B‑Cell Lymphoma. Clinical Pharmacokinetics. 2021 Dec;60(12):1621-1633. doi: 10.1007/s40262-021-01039-5. Epub 2021 Jun 14.
FDA draft guidance, March 2022: Considerations for the development of CAR-T cell products
This blog was originally published on September 9, 2022 and has since been updated.
Senior Distinguished Scientist
Rajesh is a scientific key opinion leader with 25+ years in drug development, specializing in model-informed strategies for biologics, vaccines, and small molecules. Currently a Senior Distinguished Scientist at Certara, he leads strategic consulting and the CDDS centers of excellence. Previously, he founded Merck’s quantitative clinical pharmacology department and held key roles at Aventis and Bristol-Myers Squibb. Rajesh holds a PhD in Pharmaceutical Sciences (University of British Columbia) and an MBA in Strategy and Innovation (Warwick). Consistently recognized among the top 2% of influential scientists, his work includes 100+ publications, 89 posters, and 4 books. He is an elected fellow of AAPS.

Vice President
Kathryn is a clinical pharmacology consultant and Team Lead within the Integrated Drug Development group at Certara. In addition, she leads the Complex Biologics Integrated Practice Area that specialises in providing clients with expert support in areas such as cell therapies, RNA technologies, gene therapies, fusion proteins, ADCs, bispecific antibodies, etc. Prior to joining Certara in 2020, Kathryn worked in clinical pharmacology & pharmacometrics in the pharmaceutical industry for more than 20 years, working across all phases of development.
Contact us heading