Hunter Stephens, PhDAssociate Director, Pharmacometrics
Hunter Stephens, PhDAssociate Director, Pharmacometrics Joshuaine GrantSenior Director, Quantitative Systems Pharmacology (QSP)
Joshuaine GrantSenior Director, Quantitative Systems Pharmacology (QSP) Amandine Manon, PharmDSenior Director, Clinical Pharmacology and Translational Medicine
Amandine Manon, PharmDSenior Director, Clinical Pharmacology and Translational Medicine Mirjam Trame, PharmD, PhDVice President, Certara Drug Development Solutions, Head of Pharmacometrics USA – Division II
Mirjam Trame, PharmD, PhDVice President, Certara Drug Development Solutions, Head of Pharmacometrics USA – Division IIJuly 7, 2026
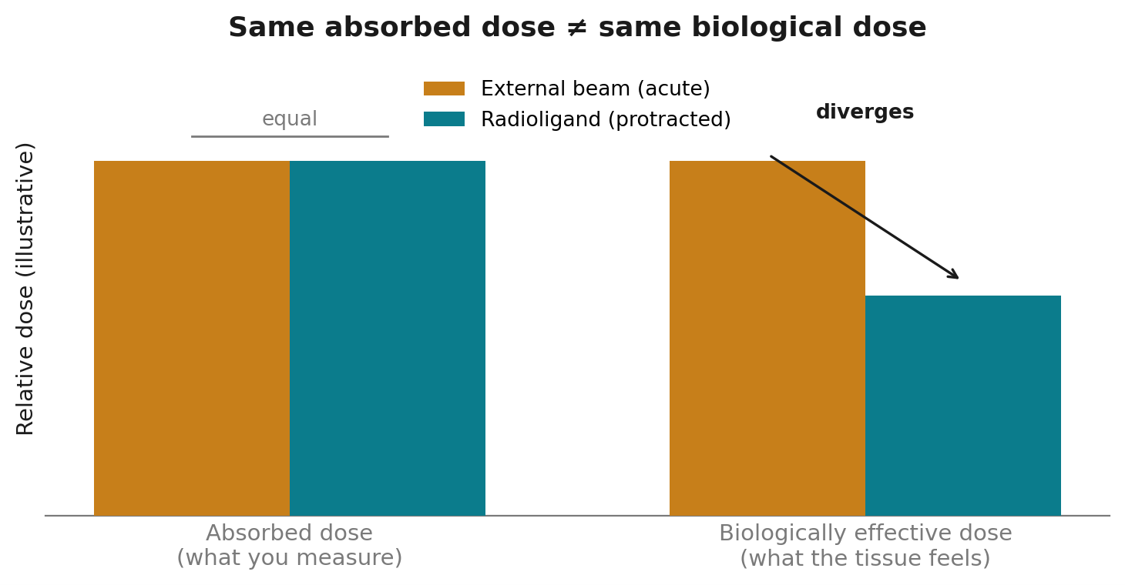
Conceptual illustration. For equal absorbed dose, a protracted low-dose-rate radioligand exposure yields a lower Biologically Effective Dose (BED) than an acute external-beam fraction — so a constraint expressed in absorbed dose does not translate between the two settings.
Advance Dose Optimization with Model-Informed Approaches
Successful radiopharmaceutical development requires more than measuring absorbed dose. Discover how Certara helps sponsors integrate dosimetry, radiobiology, pharmacometrics, and exposure-response modeling to support dose optimization and regulatory decision-making.

Sources
1. FDA. Oncology Therapeutic Radiopharmaceuticals: Dosage Optimization During Clinical Development. Draft Guidance for Industry, August 2025.
2. Dose-volume constraints for organs at risk in radioligand therapy were largely derived from external beam radiotherapy; see EBRT-derived-constraint literature in radionuclide therapy.
3. Hope TA, Hofman MS, et al. Rethinking Dosimetry: The Perils of Extrapolated EBRT Constraints to Radionuclide Therapy (editorial), J Nucl Med (2024).
4. Liubchenko G, et al. Image-based dosimetry for [225Ac]Ac-PSMA-I&T therapy and the effect of daughter-specific pharmacokinetics. Eur J Nucl Med Mol Imaging (2024). doi:10.1007/s00259-024-06681-2.
5. Response to the FDA Dosage Optimization Draft Guidance for Radiopharmaceutical Therapies, J Nucl Med (2026) — on α-emitter imaging challenges, surrogate imaging agents, and serial blood sampling for dosimetry.
—. Source poster (Certara, SNMMI): “Population Pharmacokinetic Modeling to Predict Absorbed and Biologically Effective Dose for Radioligand Therapies” (H. Stephens, A. Manon, M. N. Trame).
Hunter Stephens, PhD
Associate Director, PharmacometricsHunter Stephens, PhD, is an Associate Director in the Pharmacometrics group at Certara. He specializes in applying mathematical and computational models to understand the pharmacokinetics and pharmacodynamics of drugs, especially radiopharmaceuticals. He has a PhD in Medical Physics from Duke University. He also holds an MS in Physics from North Carolina State University and a BS in Mathematics from Tennessee Tech University. His work in TRT has focused on building semi-mechanistic population PK models to simulate and predict absorbed and biologically effective doses to inform dose-range finding and questions of safety and efficacy. In addition, he has extensive experience in radiation dosimetry from external and internal sources.
Joshuaine Grant
Senior Director, Quantitative Systems Pharmacology (QSP)Joshuaine Grant is a Senior Director in Quantitative Systems Pharmacology at Certara with more than 25 years of experience integrating biophysics, disease biology, and quantitative modeling to advance drug development. She leads collaborative projects that use mechanistic and translational QSP modeling to inform key decisions from discovery through the clinic. Her broad experience across biologics and complex therapeutics has supported Certara’s growing leadership in radioligand and targeted radiotherapies.
Amandine Manon, PharmD
Senior Director, Clinical Pharmacology and Translational MedicineAmandine joined Certara in 2020. She served as a Clinical pharmacologist in several pharmaceutical companies for 15 years. She has a proven track record in preclinical and clinical PK, clinical pharmacology with a special focus on oncology, drug development from early stages to Phase 3, and regulatory experience. Amandine graduated as a PharmD from Paris University, France and she also holds a Master’s degree in Pharmacokinetics.
Mirjam Trame, PharmD, PhD
Vice President, Certara Drug Development Solutions, Head of Pharmacometrics USA – Division IIMirjam is an expert in pharmacometrics and oncology drug development, serving as Head of Pharmacometrics USA – Division II at Certara Drug Development Solutions. With expertise spanning complex biologics, she supports exposure-response analysis, dose and study optimization, and regulatory strategy, with a special focus on radiotherapeutics and cell and gene therapies.
Advance your radiopharmaceutical development program with confidence
Whether defining your first-in-human dose, evaluating biodistribution and dosimetry, optimizing treatment strategy, or preparing for regulatory interactions, Certara helps targeted radionuclide therapy (TRT) and theranostics teams reduce uncertainty and make confident, model-informed development decisions.
We help teams